2026-07-09
Mini Facelift: Strategies for the Upper and Mid-Face
Addressing concerns about unnatural results or short-lived effects after a facelift, this article highlights the importance of tailored strategies for the upper and mid-face. It emphasizes precise diagnosis and understanding anatomical differences for optimal outcomes in procedures like forehead lifts and mini facelifts.

Mini Facelift: Strategies for the Upper and Mid-Face - Clyve Plastic Surgery -
As information about facelifts becomes more widespread, concerns such as short-lived results or an unnatural appearance after the procedure are frequently mentioned.
A significant portion of these issues stems not from the surgical technique itself, but from inaccurate diagnoses of the patient's condition and a uniform approach that fails to consider the anatomical differences of each facial region. Forehead lifts and mini facelifts, applied to the upper and mid-face respectively, should be selectively performed only after a clear understanding of their distinct structural characteristics to ensure stable results.
When surgically analyzing the face, it is useful to divide it into the lower, mid, and upper face. The lower face includes the jawline, mouth corners, marionette lines, and the border with the neck. The mid-face connects to the cheekbones, nasolabial folds, and the volume beneath the eyes, while the upper face is directly related to the forehead, eyebrows, and upper eyelids. The patterns of aging in each area are not identical, and the underlying tissues also differ.
If sagging in the mid-face is prominent, a strategy of correcting the core problem first with a mid-face lift or mini facelift may be applied before performing a more extensive facelift. Conversely, if eyebrow descent and upper eyelid skin redundancy are the primary symptoms in the upper face, adjusting the upper support structure through a forehead lift is logical. The key is to define the scope of the surgery according to the structural cause in each area; excessively including unnecessary areas can increase the surgical burden without providing significant practical benefits.
Integrated Design for Upper and Mid-Face Lifts

The upper and mid-face are anatomically continuous structures. If a forehead lift raises the eyebrows and upper structures, but mid-face sagging is not corrected, it can give the impression that the upper and middle sections are misaligned. Conversely, if only a mid-face mini facelift is performed to lift central volume, but the upper face has significant descent, the heaviness of the eyebrows and eyes will remain.
Therefore, in actual surgical planning, it is necessary to evaluate the structural problems of the upper and mid-face not in isolation, but by combining them into a single surgical plan or a staged approach.
Thus, what a good forehead lift clinic considers essential is not the name of the procedure, but rather how deep the dissection goes, which ligaments are released and re-fixed, and how the direction and strength of fixation are set. Surgery should be designed differently according to each individual's anatomy and aging pattern, and it is not advisable to limit the surgical scope without sufficient correction merely for the advantage of a minimal incision.
Precise Definition and Surgical Criteria for Mini Facelift
The term ‘mini facelift’ is used differently by various medical institutions, making it difficult for patients to understand the actual surgical content and expected effects. In some cases, even limited dissection and the insertion of lifting threads are referred to as a mini facelift. However, such approaches do not address the SMAS layer and retaining ligaments, leading to limited structural correction and potentially shorter maintenance periods.
In a strict sense, a mini facelift is not merely a reduced version, but rather a surgical technique that applies a standard SMAS facelift, focused on the mid-face, with a more reasonable scope and incision. This is a more appropriate understanding.
A clinic specializing in forehead lifts typically accesses the mid-face SMAS layer, partially resects and releases the retaining ligaments in the cheekbone and cheek areas, repositions the malar fat pad and soft tissues superolaterally, and, if necessary, refines the contour of a portion of the jawline.
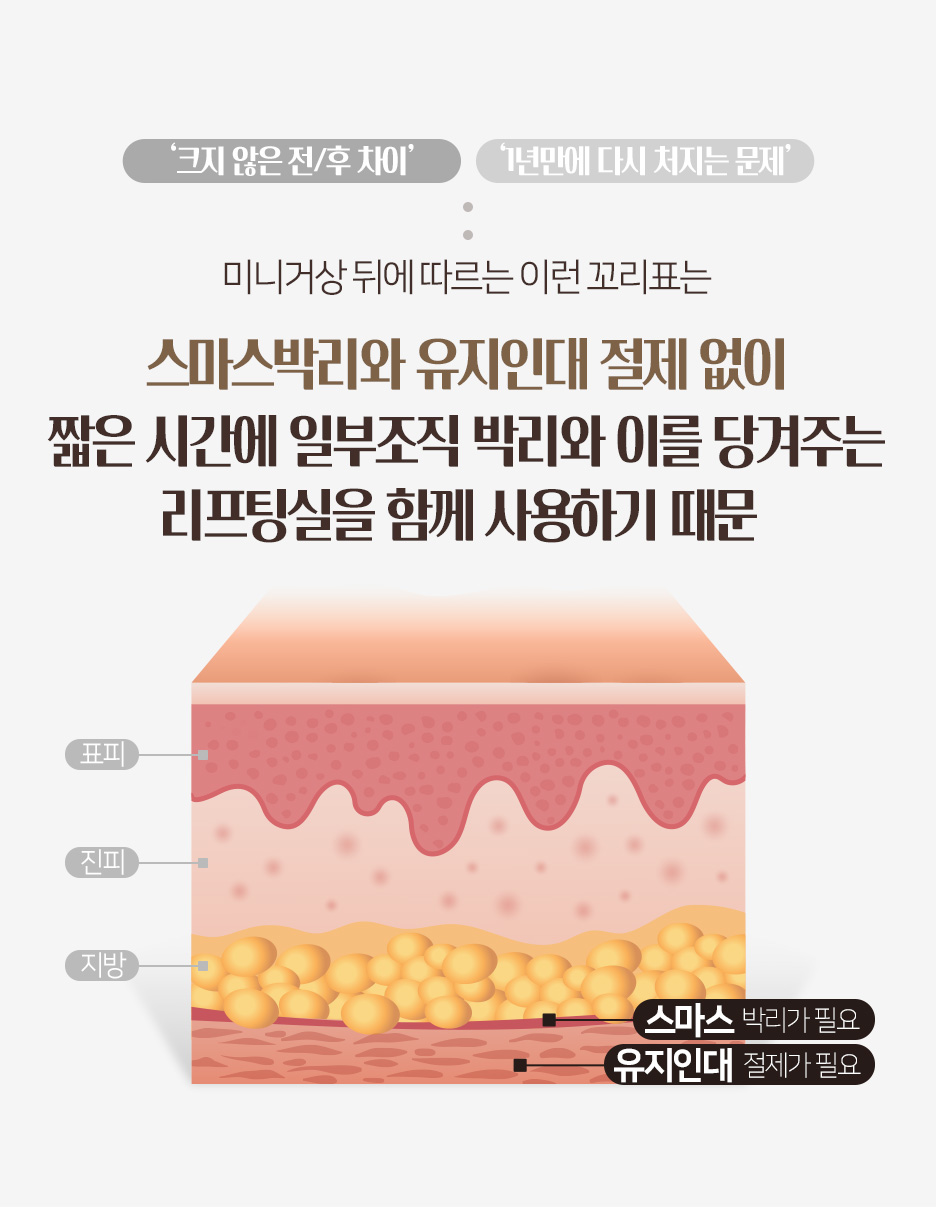
When these structural elements are included, a clear difference before and after the procedure is evident, and durability is also secured, even within a limited incision range. Conversely, if only thread lifting is performed without SMAS layer dissection, the likelihood of re-sagging within several months may increase.
Therefore, when looking for a clinic that performs good forehead lifts, it is crucial to specifically confirm whether SMAS dissection and retaining ligament management are included in the actual surgical plan.
It is also necessary to differentiate approaches based on age and skin condition. For early stages of sagging, typically in the late 30s to early 40s, sufficient improvement can be achieved with micro-correction focused on the mid-face rather than extensive dissection. In contrast, for those in their late 40s and beyond, where SMAS laxity and ligament deformation are evident, even a mini facelift should involve fascial fixation and ligament repositioning to ensure structural stability.
The term ‘mini’ can be used to describe the incision range and recovery burden, but the depth of correction and anatomical completeness should not be compromised.
Structural Design and Fixation Methods for Forehead Lifts

A forehead lift is a surgery that adjusts the overall impression of the upper face, requiring consideration of the forehead skin and soft tissues, eyebrow position, amount of excess skin on the upper eyelids, and the tension of the glabellar muscles. If one attempts to resolve upper facial aging solely by excising upper eyelid skin, eyebrow descent and forehead heaviness may remain, potentially exacerbating functional problems. A forehead lift views the entire upper face as a single functional unit, reconstructing the periosteum, fascia, muscles, and skin in a consistent direction.
The surgery is performed through an incision within the scalp or at the hairline, dissecting along the galea aponeurotica and subperiosteal layer to release the retaining ligaments that pull down the eyebrows and forehead. Subsequently, the dissected tissues are repositioned and fixed upwards or superolaterally. The fixation method at this stage is directly related to the stability of the surgical outcome.
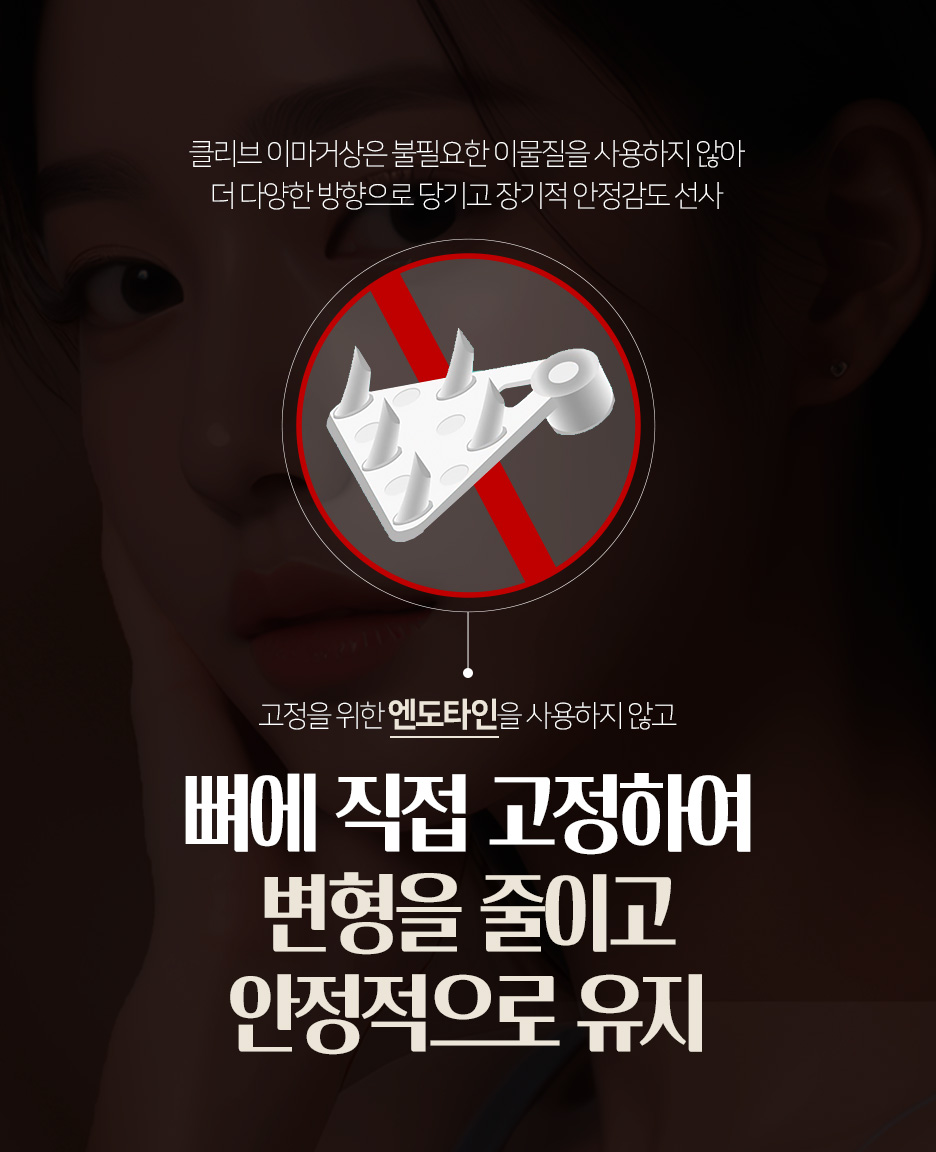
Auxiliary fixation devices like Endotine can support tissues for a certain period, but it is also considered that in specific situations, issues such as residues, palpable sensation, and problems during revision surgery may arise. Consequently, some practitioners adopt a method of direct periosteal fixation with sutures, without using implants.
While this method requires skilled surgical techniques, it offers clear fixation points and allows for the design of traction vectors in various directions, which is advantageous for precise adjustment of the upper facial line.
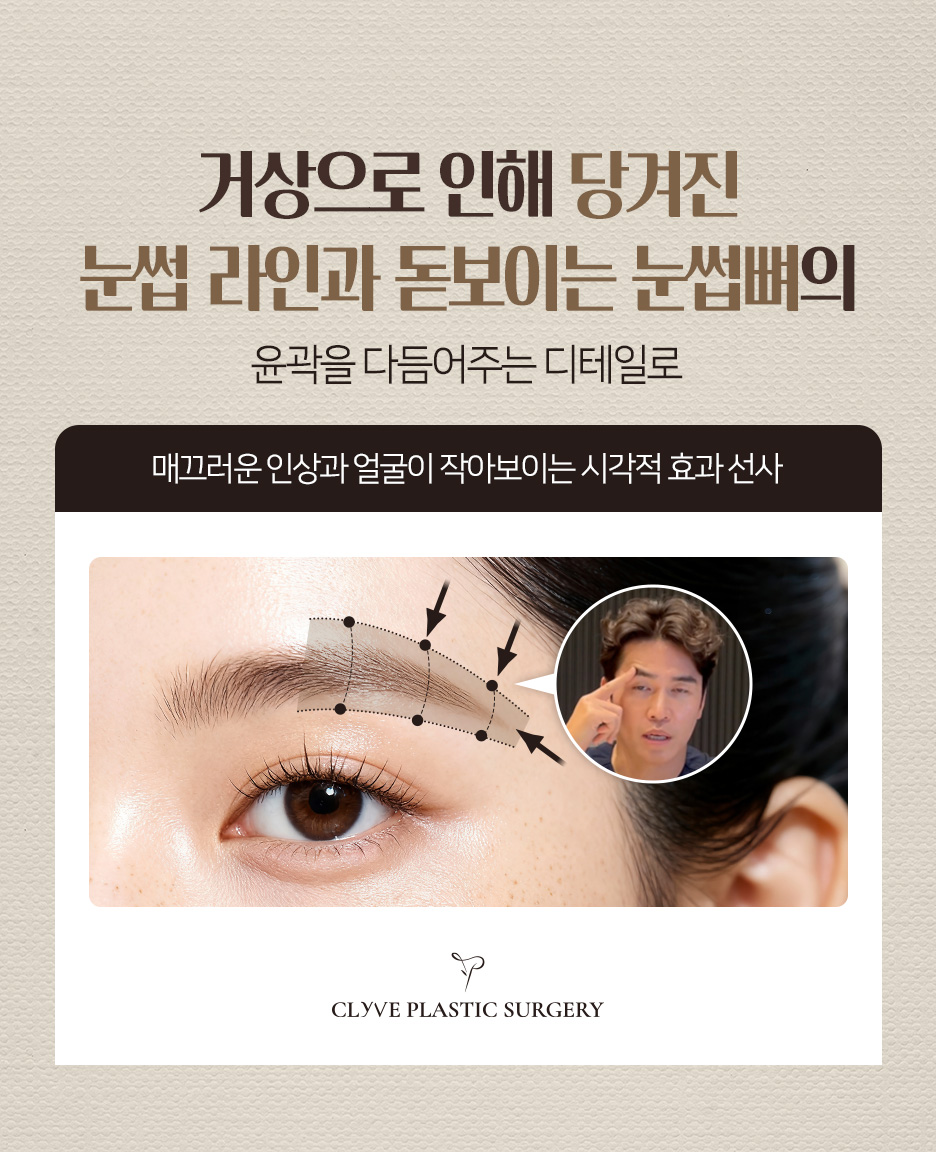
A crucial variable in a forehead lift is the final position and curve of the eyebrows. If the eyebrows are fixed excessively high, the forehead may appear wider or the expression sharper; if only the outer corners are excessively raised, it can be perceived as an unnatural expression.
Therefore, the key is to adjust the medial, central, and lateral points of the eyebrows with different tensions and directions to form a curve that harmonizes with the existing facial structure. Additionally, the upper orbital bone contour, which might appear prominent, should ideally be visually refined through the redistribution of surrounding soft tissues.
Both forehead lifts and mini facelifts are effective surgical tools for correcting aging in the upper and mid-face. However, the essence of these two surgeries is not a ‘simple lift,’ but rather a structural redesign based on functional and aesthetic correction of the complex upper face (forehead, eyebrows, upper eyelids), and restoration of volume and contour through the repositioning of the mid-face SMAS layer, retaining ligaments, and fat pads.
In other words, a reliable surgical design is not a matter of ‘which is better, a forehead lift or a mini facelift,’ but rather determined by a specific plan that analyzes the individual patient's upper and mid-face anatomy, age, elasticity, and ligament condition to decide which layers and areas to correct, and in what direction. Where such a plan is clearly explained, more stable lifting results can be expected.




Mini Facelift: Strategies for the Upper and Mid-Face

Mini Facelift: Strategies for the Upper and Mid-Face










Mini Facelift: Strategies for the Upper and Mid-Face










Frequently Asked Questions
Why do facelifts sometimes result in an unnatural look or short-lived effects?
This primarily stems from inaccurate diagnoses of the patient's condition and a uniform approach that fails to consider the anatomical differences of each facial region. It is crucial to accurately identify the aging patterns and underlying tissues of each area and plan a customized surgery.
What exactly is a mini facelift?
A mini facelift is a surgical technique that applies a standard SMAS facelift, focused on the mid-face, with a reasonable scope and incision. It should involve structural correction, including accessing the SMAS layer, partially resecting retaining ligaments, and repositioning soft tissues, not just simple thread insertion.
What should I check when choosing a clinic for a mini facelift?
It is important to specifically confirm whether SMAS layer dissection and retaining ligament management are included in the actual surgical plan. If only thread lifting is performed without SMAS layer dissection, the likelihood of re-sagging within several months may increase.
How are the upper and mid-face considered together in surgery?
The upper and mid-face are anatomically continuous structures. Therefore, in actual surgical planning, it is necessary to evaluate the structural problems of each area and then combine them into a single surgical plan or a staged approach. Achieving harmony from an integrated perspective is crucial.
What is the most important aspect of a forehead lift?
A crucial variable in a forehead lift is the final position and curve of the eyebrows. If the eyebrows are fixed excessively high or only the outer corners are raised, it can appear unnatural. Therefore, the key is to delicately adjust the medial, central, and lateral points of the eyebrows with different tensions and directions to form a curve that harmonizes with the existing facial structure.